HIE: Clinical Information Reconciliation
Click the following dropdowns to see what's changed for this measure.
The following table includes this measure's changes for 2020.
| Measure Changes for 2020 | |
|---|---|
| Name Changes | None |
| Measure Changes |
None |
| Workflow Changes |
None |
The following table includes what changed for this measure in 2019.
| Measure Changes for 2019 | |
|---|---|
| Name Changes |
None |
| Measure Changes |
This documentation has been modified to reflect that the numerator and denominator count referrals, rather than visits. |
| Workflow Changes |
Importing the Electronic Summary of Care Document Previously, the practice could save the CCDA document as a Clinical Document, which had to be linked to the qualifying visit. For 2019, you must save the CCDA document as a Reference Document. Reference Documents do not need to be linked to a visit when they are saved. However, you must link the document to a visit when automatically reconciling data. |
|
Reconciling Data Manually from the Facesheet Link the visit in the buffer before starting the reconciliation. After you manually reconcile using the History & Habits Wizard or Medications List, rather than a Note, you must create or edit the visit's Note. You must then load the PFSH, Assessment, and Plan sections to record the reconciliations in the Note. |
|
|
Reconciling Data Automatically by Importing In the Clinical Reconciliation window, you must select at least one item under Demographics, along with any items from the Allergy, Medications, and Problem List sections, before selecting the Import button. |
|
Measure Overview
This measure reports the referral or transitions of care in which a patient is seen for the first time, referred into the practice, or is an existing patient who already has a summary of care document saved to their chart, and the provider performs a clinical information reconciliation using the information from the patient or from an electronic summary of care document, including the following three clinical information sets: Medication, Medication Allergy, and Current Problem list.
| Measure Overview | |
|---|---|
| Denominator | The number of transitions of care or referrals into the practice for which the EP was the recipient of the transition or referral or has never before encountered the patient. |
| Numerator | The number of referrals or transitions of care that qualified for the denominator where the EP performed a reconciliation of medications, medication allergies, and current problems. |
| Medicaid Goal |
Must Exceed 80% |
See the following sections for more information on the HIE: Clinical Information Reconciliation measure:
- Denominator Criteria
- Numerator Criteria
- Setup Requirements
- HIE: Clinical Information Reconciliation Workflows
Denominator Criteria
Transitions of care or referrals qualify for the denominator if they occur during the measurement period. This can be indicated by any of the following:
- New Patient Visit: The Plan or E&M section of the Note includes a new patient E&M code for the patient. New patient E&M codes include codes in the range of 99201-99205 or 99381-99387. This Note must be linked to a visit that occurred during the measurement period, and the code must be added at the same time or after the start of the visit.
- Referral or Transition into the Practice: The Inbound Referral/Transition check box is selected under Referrals in the Plan section of the Note. This Note must be linked to a visit that occurred during the measurement period, and the check box must be selected at the same time or after the start of the visit.
- Summary of Care Record: An electronic summary of care document (also known as a CCD or continuity of care document) is in the Reference Documents section on the patient’s Facesheet. The import date for this document can be any time before the end of the visit, even before the start of the measurement year. The document must be linked to the visit.
All denominator criteria must be met during the measurement period set in Prime Suite Reporting 2020.
Numerator Criteria
To qualify a transition of care or referral for the numerator, providers must perform three reconciliations of clinical data for the patient during the same visit. These three reconciliations include:
- Medications: Review of the patient’s medications. When documenting medications, CMS requires the name, dosage, frequency, and route of each medication to be collected. In the event of an audit, it is the site’s responsibility to ensure this information is documented for the patient’s outside medications.
- Medication Allergies: Review of the patient’s allergies for known medication allergies.
- Current Problems: Review of the patient’s problems for current and active diagnoses.
When documenting these three reconciliations, the provider is indicating they occurred during a face-to-face visit with the patient.
To qualify for the numerator when performing these reconciliations, all the following are required:
- The provider performed a Medications, Medication Allergies, and Current Problems reconciliation during the same visit.
- The visit used to perform the reconciliations is the patient’s first visit and occurred during the measurement period set in Prime Suite Reporting 2020.
- The reconciliations occurred during or after the visit was checked-in and linked but within the measurement period set in Prime Suite Reporting 2020.
- The patient's summary of care document is linked to the qualifying visit when automatically reconciling data.
All the above numerator actions must be completed during the calendar year that the measurement period begins in. For example, if the measurement period begins on 3/3/2020, the numerator must be met during the period that begins on January 1, 2020 and ends on December 31, 2020.
Setup Requirements
See the following sections for this measure's setup requirements:
- Setting the Reconcile Reference Documents User Right
- Adding the Reference Documents Section to the Facesheet
- Configuring the Method by Which Your Organization Will Import CCDs
Setting the Reconcile Reference Documents User Right
Users must have the Reconcile Reference Documents user right assigned before they can automatically reconcile CCDAs. To grant users this permission, follow these steps:
| 1. | Select System > User Rights. The User Rights window opens. |
| 2. | Select System under Modules on the left-hand side. |
| 3. | Select Reference Documents under System Categories. |
| 4. | Select the check box for Reconcile Reference Documents. |
| 5. | Select Save under Category Actions on the left-hand side to save your changes. |
Adding the Reference Documents Section to the Facesheet
The Reference Documents section allows you to receive CCDA documents from external sources and add them to a patient’s Facesheet without importing the information directly into the chart. Although you can add documents to the Reference Documents when the section is not included on the Facesheet, it does make the process easier.
| 1. | Open the Chart menu and select User Settings Admin. |
| 2. | Select the Facesheet & History tab. |
| 3. | Scroll down to Facesheet Sections. |
| 4. | Select the Reference Documents check box. |
| 5. | Select Save. |
| 6. | On the Facesheet, select Customize Facesheet and select the Reference Documents check box to add this section. |
Configuring the Method by Which Your Organization Will Import CCDs
You must configure the method by which your organization will import CCDs. You can set this by following these steps:
| 1. | Open the System menu and select System Defaults. |
| 2. | Select the Chart Defaults tab. |
| 3. | Scroll down to the External Document Default Actions section and select the Action Admin link. |
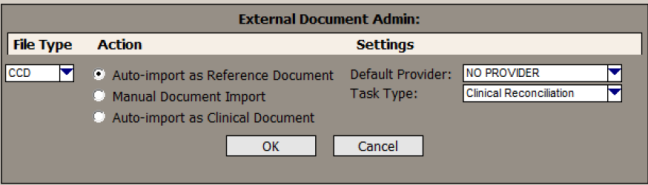
| 4. | Select CCD in the File Type list. |
| 5. | Select from the following radio buttons in the Action section: |
- Auto-import as Reference Document: Selecting this option imports all CCDs to the Reference Documents section of the Facesheet. This gives users the ability to electronically reconcile each CCD. Additionally, this setting prevents users from skipping reconciling and saving the CCD directly to the chart.
- Manual Document Import: Selecting this option allows users to either save CCDs to the Reference Documents section of the Facesheet or directly into the chart. This option should be selected if users should have the option of reconciling a CCD.
- Auto-import as Clinical Document: Selecting this option saves all CCDs directly into the patient’s chart. With this selection, there is no opportunity to electronically reconcile the information contained in the CCD.
The Auto-import as Clinical Document option will not qualify visits for this measure.
| 6. | Select OK to save your changes or select Cancel to return to the Chart Defaults tab without saving the changes. |
| 7. | Select Save on the Chart Defaults tab to save all the changes made. Alternatively, select Cancel to discard your changes. |
HIE Clinical Information Reconciliation Workflows
You can reconcile information that comes from the patient or from their electronic summary of care documents.
- You must manually reconcile data that comes from the patient or their representatives. After performing the needed reconciliations, you must add related information to the visit’s note.
- You can automatically reconcile a CCDA that has been saved to the Reference Documents section of a patient’s chart.
See the following sections for more information on reconciling patient information:
Manually Reconciling Data
You can manually reconcile Medications, Medication Allergies, and Problems using the History & Habits Wizard, the Medications List, or a Note. Be aware of the following:
- Reconciling from the History & Habits Wizard or the Medications List must be done while linked to the visit that qualified for the denominator. Additionally, after reconciling the needed data, you must include the reconciled data in a Note.
- When manually reconciling in a Note, Allergies are reconciled in the PFSH section, Problems are reconciled in the Assessment section, and Medications are reconciled in the Plan section. When reconciling in a Note, it must be linked to the visits that qualified for the denominator.
Prior to starting the reconciliations, make sure that the visit is selected in the top left of Prime Suite for the reconciliation to be associated with the visit.
See the following sections for more information on manually reconciling data:
- Manually Reconciling Allergies
- Manually Reconciling Problems
- Manually Reconciling Medications
- Including Reconciled Data in a Clinical Note
Manually Reconciling Allergies
| 1. | In the Allergy section of the History & Habits Wizard or the PSFH section of the Note, manually compare the patient’s data from the Summary of Care to the data in Prime Suite. |
| 2. | Update Prime Suite as necessary based on your comparison. |
| 3. | Document that you performed the reconciliation: |
- In the History & Habits Wizard, select the Allergies Reconciled check box in the Allergy section.
- In the PFSH section of a Note, select the Allergies Reconciled check box.
By selecting one of these check boxes, the provider is indicating that the reconciliation occurred during a face-to-face visit.
Manually Reconciling Problems
| 1. | In the Problems section of the History & Habits Wizard or the Assessment section of the Note, manually compare the patient’s data from the Summary of Care to the data in Prime Suite. |
| 2. | Update Prime Suite as necessary based on your comparison. |
| 3. | Document that you performed the reconciliation: |
- In the History & Habits Wizard, select the Problems Reconciled check box in the Problems section.
- In the Assessment section of a Note, select the Problems Reconciled check box.
By selecting one of these check boxes, the provider is indicating that the reconciliation occurred during a face-to-face visit.
Manually Reconciling Medications
| 1. | In the Meds section of the History & Habits Wizard, the Medication List, or the Plan section of the Note, manually compare the patient’s data from the Summary of Care to the data in Prime Suite. |
| 2. | Update Prime Suite as necessary based on your comparison. |
| 3. | Document that you performed the reconciliation: |
- In the History & Habits Wizard, select the Reconciled Medications check box in the Meds section.
- In the Medication List, select the Reconciled Medications check box.
- In the Plan section of a Note, select the Medications have been Reconciled check box.
While in the Plan section, make sure that the Inbound Referral/Transition check box is selected if the patient was referred or transitioned into the practice.
By selecting one of these check boxes, the provider is indicating that the reconciliation occurred during a face-to-face visit.
If you used the History & Habits Wizard or Medication List to reconcile the data, you must also include the reconciled data in a clinical Note on the visit. If you don’t include this data in a Note, the reconciliations will not be properly recorded and will not qualify. See Including Reconciled Data in a Clinical Note below for more information.
Including Reconciled Data in a Clinical Note
| 1. | After performing the medications, allergies, and problems reconciliations, create or edit the visit's Note. |
| 2. | Select and load the following sections in the Note: |
- PFSH: To include the allergy reconciliation.
- Assessment: To include the problem reconciliation.
- Plan: To include the medication reconciliation.
As you load each section, the corresponding reconciled information is pulled from the History & Habits Wizard or the Facesheet into the Note and, as long as you selected the reconciled check boxes, the Allergies Reconciled, Problems Reconciled, and Medications have been Reconciled check boxes are automatically selected.
While in the Plan section, make sure that the Inbound Referral/Transition check box is selected if the patient was referred or transitioned into the practice.
| 3. | Verify the Allergies Reconciled, Problems Reconciled, and Medications have been Reconciled check boxes are selected. |
| 4. | Save the note. |
Automatically Reconciling a CCDA
When a CCDA is in the Reference Documents section of a patient’s chart, you can import data from the CCDA to automatically reconcile its data to the patient’s chart. When automatically reconciling, the selected medication, allergy, and problem data is added into the patient’s chart and marked as reconciled at the same time.
You must select at least one item under Demographics, before launching the Import.
Users must have the Reconcile Reference Documents user right assigned to automatically reconcile CCDAs. See Setup Requirements above for more information.
To automatically reconcile a CCDA:
| 1. | Link the visit prior to doing the reconciliation. You should use the visit associated with the transition of care. |
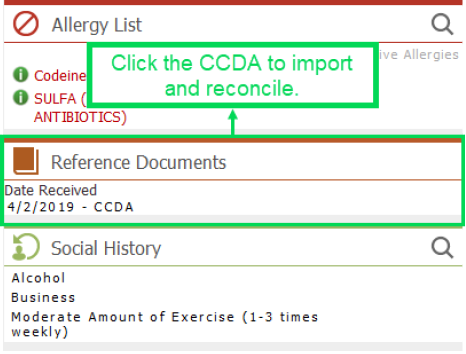
| 2. | In the Reference Documents section of the patient's Facesheet, select the CCDA you want to reconcile to load it in the Reference Document Viewer. |

Verify that the VisitID number in the Reference Document Viewer matches the Visit ID number in the Global Visit buffer before Reconciliation/Incorporation.
| 3. | Link the visit to the CCDA before starting the reconciliation: |
| a. | Select Select Visit to open the Visit Search window. The patient’s identification number is displayed in the Patient ID field. |
| b. | Select Search to find all of the patient's visits. |
| c. | Select the visit associated with the transition of care, and then select OK to confirm that you want to associate the selected visit with the document and return to the Reference Document Viewer. |
This must match the currently linked visit.
| 4. | Select Reconcile to open the Clinical Reconciliation dialog box. This dialog box includes sections that allow you to compare content from the CCD with content from the patient’s chart. |

Data from the patient’s chart displays in the From Patient’s Chart Facesheet column on the left-hand side. Data from the CCD displays in the From Clinical Summary column on the right-hand side. If information from the CCD differs from the patient’s chart, the new information displays as a selectable hyperlink in red text.
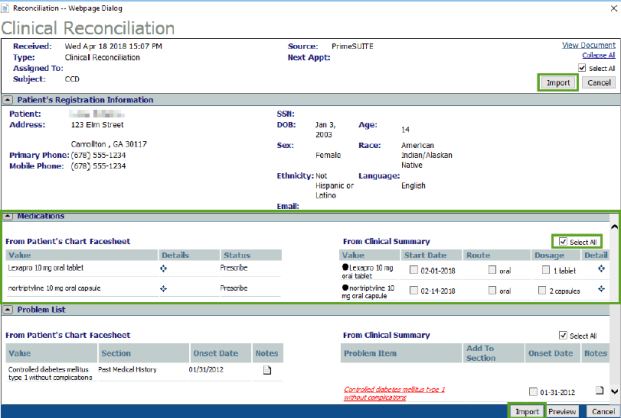
| 5. | Compare and evaluate the contents of the Medications, Problem List, and Allergy sections. |
| 6. | New patient information on the CCDA indicated by a red hyperlink must be mapped to an existing item on the patient's facesheet or imported without mapping to be included in the patient's chart. Select the red hyperlink for a new item to open the Facesheet Section Search dialog box. |
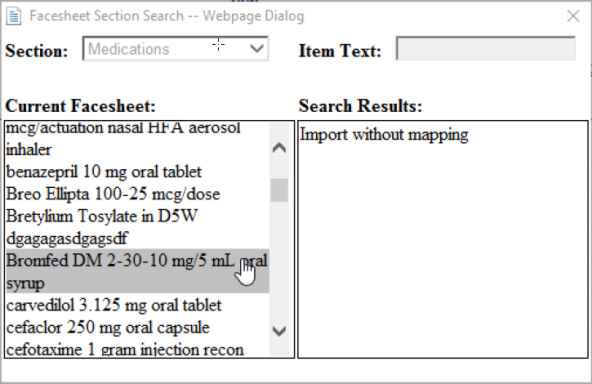
| 7. | Map the selected item from the CCD to an item on the Patient’s Facesheet by selecting an item in the Current Facesheet column. Alternatively, you can select Import without mapping in the Search Results column. |
| 8. | Repeat Steps 5-6 for any new items on the CCD indicated by a red hyperlink to either map the item or import the item to the patient’s Facesheet without mapping. |
| 9. | Use the check boxes in the From Clinical Summary pane of each section to select the data to import into the patient’s chart. To include all the information from the clinical summary in the patient’s chart, select the Select All check box. |
The Select All check box will not automatically import the new information for the patient in the CCDA indicated by red hyperlinks. You must select these and choose how to import this information.
| 10. | Select at least one item under Demographics in the Clinical Reconciliation window before selecting the Import button. If no demographic information needs to be updated, you must select the Select All check box in the Demographics section. |

If you do not update any demographic information or select the Select All check box, the referral will not qualify for the numerator.
| 11. | After selecting all of the desired information to import, select Import. |
The selected data is imported into the patient chart and the Medication List, Allergy List, and Problem List. This data will be marked as Reconciled in the database.
| 12. | Select OK to dismiss the success notification message once the import completes. |


